You notice a sore after practice, or your child points to a “spider bite” that wasn't there yesterday. It's red, swollen, tender, and somehow seems more painful than it looks. That's often the moment people search for MRSA infection signs and worry they're already behind.
A calm response helps more than panic. MRSA can start as a skin problem that looks ordinary at first, but some signs deserve quick medical attention. Just as important, a positive MRSA test doesn't always mean someone has an active infection. That distinction matters in homes, schools, locker rooms, and healthcare settings.
What is MRSA and Why is It a Concern
A child comes home from practice with a sore on the leg. A gym member notices a tender bump after using shared equipment. The hard part is that the word "MRSA" can make people jump to two wrong conclusions at once. Some assume every red bump is a dangerous infection. Others hear that someone "has MRSA" and do not realize that a person can carry the bacteria without being sick.
That distinction matters.
MRSA is a type of staph bacteria that resists several antibiotics commonly used for ordinary staph infections. The bacteria may live on the skin or in the nose without causing symptoms. That state is called colonization. An active infection means the bacteria have moved from being present to causing damage, such as a painful skin lesion, drainage, fever, or a deeper illness.
Why people worry about it
People worry about MRSA for a practical reason. If an active infection is missed, it can spread into deeper tissue or, in more serious cases, into the blood, lungs, or other parts of the body. In healthcare settings, MRSA also spreads more easily because people may have wounds, medical devices, or weakened immune systems. If you are also trying to understand infections picked up in medical settings, this overview of hospital-acquired infection basics may help.
At the same time, panic creates its own problems. Families may treat colonization like an emergency. Schools and gyms may overreact to the label but miss the everyday hygiene steps that reduce spread. MRSA works a bit like a spark near dry grass. A spark sitting on concrete may do nothing. A spark in the wrong place can start a fire.
Practical rule: The label matters less than the symptoms. Carrying MRSA is different from having a painful, draining, or rapidly worsening infection.
Where MRSA is commonly found
MRSA shows up in two broad settings. One is the community, including households, schools, locker rooms, and gyms, where close skin contact, shared items, and small cuts are common. The other is healthcare, where exposure risk is higher for people with surgery sites, catheters, chronic wounds, or longer hospital stays.
This is why MRSA gets so much attention. It is common enough to appear in ordinary places, but serious enough that a true infection should not be brushed off. The goal is not to fear every bump. The goal is to recognize when bacteria are being carried, when they are causing an active infection, and when hygiene and medical care need to step in.
Identifying Early MRSA Infection Signs on the Skin
A child comes home from practice with what looks like a bug bite on the leg. By the next day, the spot is more painful, warmer, and starting to swell. That kind of fast change is one reason MRSA skin infections get missed at first.

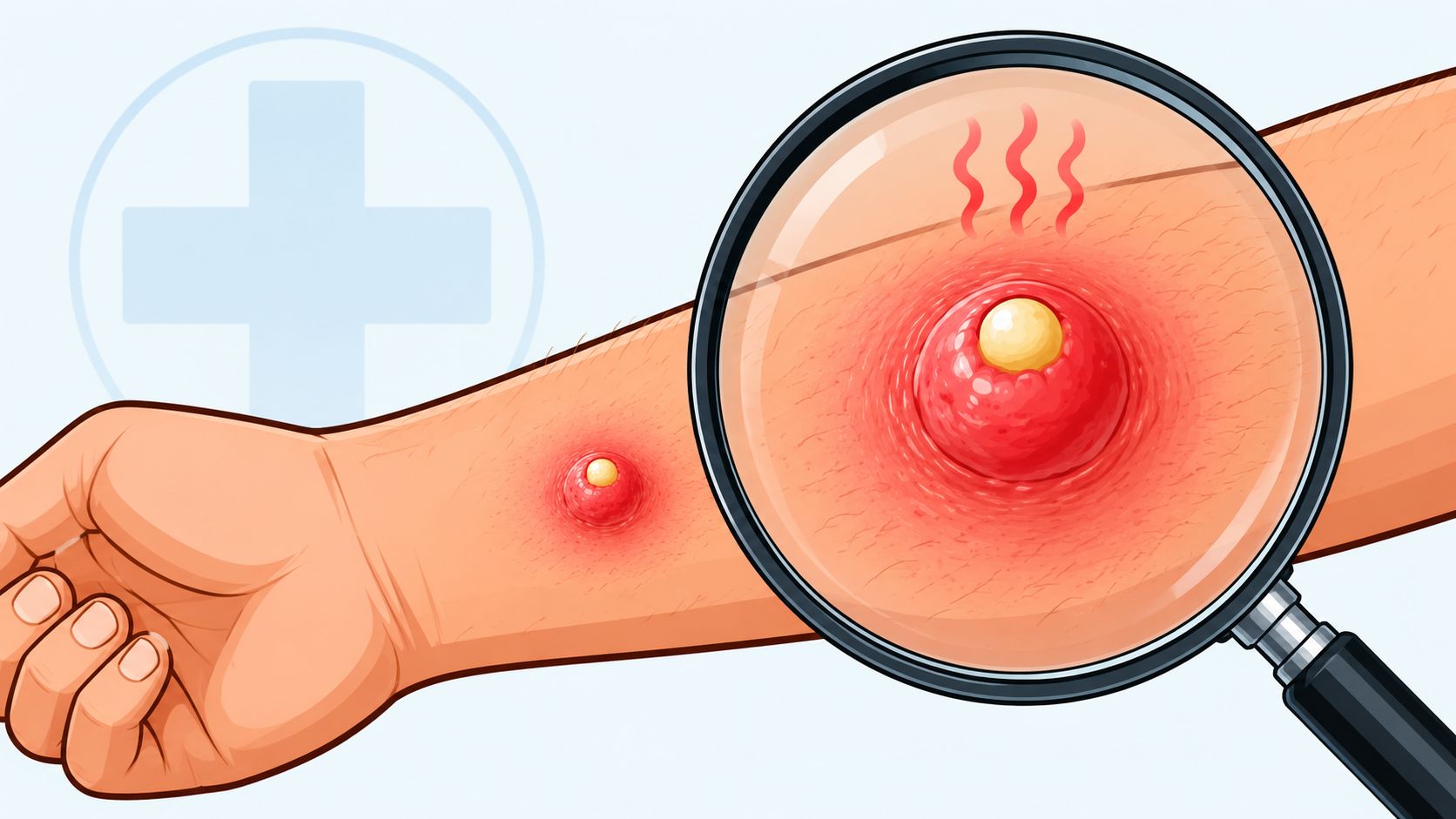
MRSA on the skin often starts as a small red bump that resembles a pimple, ingrown hair, boil, or spider bite. The problem is not the label someone gives it on day one. The problem is the pattern. An active infection usually becomes more inflamed, more tender, and more noticeable over a short time. By contrast, a person can carry MRSA on the skin or in the nose and have no sore, no pain, and no visible skin changes at all. Carrying the bacteria is colonization. A painful, worsening bump points more toward infection.
What the spot usually looks and feels like
A suspicious lesion often shows several signs together, not just one. The area may look red and puffy. It may feel firm or swollen, warmer than the skin around it, and sore enough that touching it gets your attention. Many people also notice a yellow or white center, or fluid draining from the spot.
If you are not sure whether you are seeing mild irritation or a stronger inflammatory response, these signs of inflammation can help you judge what is changing in the skin.
Pain that seems bigger than the spot looks is another clue. A simple pimple can be annoying. A possible MRSA lesion often feels more like pressure building under the skin.
How it tends to change over a short time
Speed matters here. A routine blemish usually follows a familiar, slower course. A possible MRSA infection often gets larger, redder, hotter, or more painful within a day or two.
Parents often describe it in plain language. “Yesterday it looked minor. Today it looks infected.” Gym owners and coaches hear the same story after turf burns, shaving nicks, or skin-to-skin contact. Any area with broken skin deserves a closer look, especially if the person also feels unwell.
If a “spider bite” keeps getting redder, hotter, and more painful instead of calming down, it needs attention.
Common ways people misread early MRSA
Early MRSA is easy to underestimate because it can copy everyday skin problems. People often describe it as:
- A pimple that is unusually painful
- A boil that throbs or feels tight
- A bite-like bump that keeps expanding
- A sore with a soft, pus-filled center
- A small wound that starts draining
One more point causes confusion. Putting antibiotic ointment on every suspicious bump does not confirm what it is, and skin products can sometimes irritate the area or cause a reaction of their own. If you use over-the-counter treatment, it helps to know the bacitracin side effects explained.
The main takeaway is simple. Visible skin changes suggest an active problem on the skin. No symptoms at all suggest colonization may be the issue instead. That distinction helps families and facilities respond calmly, clean shared surfaces, cover draining wounds, and seek medical care when a sore is clearly getting worse.
Is It a MRSA Bump or Something Else
There's no need for undue fear; a clearer comparison is required. A possible MRSA spot can overlap with acne, irritation, or an insect bite, but the pattern is often different.
MRSA vs. Common Skin Bumps
| Symptom | MRSA Lesion | Pimple / Acne | Spider Bite |
|---|---|---|---|
| Pain level | Often noticeably painful and tender | Usually mild to moderate soreness | Can sting or itch, sometimes painful |
| Speed of change | Often gets worse quickly | Usually develops more gradually | Often noticed suddenly, then may stabilize |
| Warmth | Commonly warm to the touch | Less often distinctly hot | May be irritated, but not always hot |
| Pus or drainage | Frequently develops pus or drainage | May have a whitehead, but often smaller and more limited | Usually not a pus-filled boil early on |
| Overall appearance | Red, swollen, inflamed bump or boil | Surface blemish or clogged pore | Bite-like spot, often with itch or local irritation |
| When to worry | If enlarging, very painful, or draining | If unusually inflamed or widespread | If worsening instead of improving |
A useful question to ask
Ask yourself this. Does the pain and inflammation seem out of proportion to what the bump looks like? That's a common reason people move from “I'll watch it” to “this needs medical advice.”
A second clue is behavior. Pimples usually follow a familiar pattern. A suspected MRSA lesion often doesn't. It becomes hotter, fuller, and more painful, and the surrounding skin may start looking increasingly inflamed.
If you're deciding whether to put ointment on a suspicious sore, it also helps to know that topical products can irritate skin or trigger reactions in some people. This guide on bacitracin side effects explained gives useful context before you apply anything to an already inflamed area.
Don't squeeze, lance, or pop a suspected MRSA boil at home. That can worsen tissue injury and increase the chance of spread.
When MRSA Becomes a Medical Emergency
Most MRSA concerns begin with the skin. The danger changes when the whole body starts showing signs that the infection may be spreading.

The CDC notes that systemic signs of MRSA include fever of 100.4°F or 38°C or higher, chills, and confusion. It also states that red streaks branching outward from a lesion can indicate spread to the bloodstream and require immediate medical intervention, and that MRSA can cause more aggressive tissue destruction than methicillin-sensitive Staphylococcus aureus because of its resistance profile (CDC overview of MRSA warning signs).
Red flags that change the situation
Seek urgent medical care if a person with a suspicious skin infection develops:
- Fever or chills
- Dizziness
- Confusion
- Muscle pain
- Red streaks spreading away from the sore
- Shortness of breath
- Rapidly expanding redness
- Severe worsening pain
These signs matter because they suggest the problem may no longer be limited to the skin.
Why these signs are more serious
A localized boil is one problem. A spreading infection is a different one. Once bacteria move beyond the original site, the body can react in ways that become dangerous quickly, especially if treatment is delayed.
That's why a “wait and see” approach stops being reasonable when the person seems sick overall, not just sore at one spot.
A painful draining lesion plus fever is not a home-care problem.
For gym operators, school nurses, and caregivers, this is the threshold to act firmly. Isolate shared personal items, avoid direct skin contact, and get the person evaluated rather than trying another round of home remedies.
Colonized vs Infected Understanding Your MRSA Status
Many families and facility managers frequently misunderstand the distinction. Colonized and infected do not mean the same thing.
A person who is colonized carries MRSA on the skin or in the nose without signs of illness. A person who is infected has symptoms, such as a painful draining lesion, fever, or other signs of active disease.
Why a positive test can be confusing
Cleveland Clinic notes that over 30% of the population carries Staph aureus asymptomatically, and about 2% carry MRSA specifically without active infection. It also explains that people often confuse colonization with disease, even though colonization rarely requires treatment but does call for strict hygiene precautions (Cleveland Clinic on MRSA colonization and infection).
That means a child who tests positive but has no rash, no fever, no painful boil, and no draining wound is not automatically “sick with MRSA.” The situation still matters, but the response is different.
What colonization means in practical terms
Colonization means:
- The bacteria may be present without causing symptoms
- The person can still spread it through poor hygiene or wound contact
- Routine hygiene becomes especially important
- Antibiotics are not automatically the answer
For schools, teams, and households, this distinction lowers panic and sharpens action. You don't need to treat every positive screen like an emergency. You do need to take hand hygiene, wound covering, and shared-item rules seriously.
How to Prevent and Control MRSA Spread
A common mistake in homes, schools, and gyms is treating every MRSA concern the same way. The better approach is to control the routes of spread. MRSA moves most easily where people are close together, skin is damaged, hygiene slips, and shared items or surfaces carry germs from one person to another. CDC describes these risk conditions as the five Cs: crowding, skin-to-skin contact, compromised skin, contaminated items and surfaces, and lack of cleanliness (CDC on MRSA prevention in community settings).

Prevention works like blocking exits in a fire drill. If you cover draining skin, clean hands, avoid sharing personal items, and disinfect surfaces correctly, you remove the main ways MRSA spreads.
What parents and caregivers should do
At home, focus on habits that interrupt contact with wound drainage and used personal items.
- Keep cuts and draining areas covered: Use a clean, dry bandage and change it as needed.
- Do not share personal items: Towels, razors, washcloths, clothing, and sports gear can pass bacteria from skin to skin.
- Wash hands after bandage changes: Soap and water work well. Alcohol-based hand sanitizer can help when hands are not visibly dirty.
- Launder soiled items promptly: Wash towels, bedding, and clothes that touch the affected skin.
- Pay attention to skin changes: A spot that becomes more painful, swollen, warm, or starts draining needs medical attention.
For families trying to understand how these exposures start, this guide to what causes MRSA infections gives useful background.
What gyms, schools, and facility managers should do
Shared spaces need a written routine that staff can follow. A quick daily wipe is often not enough if equipment is used back to back or if people with uncovered wounds are participating.
- Clean high-touch surfaces on a schedule: Mats, weight benches, locker handles, training pads, and shared equipment need consistent attention.
- Use an EPA-registered disinfectant as directed: The label matters. It tells you whether the product is appropriate and how long the surface must stay wet.
- Pre-clean visible dirt or sweat first: Disinfectants work poorly on a dirty surface.
- Train staff on contact time: If the surface dries too soon, the product may not work as intended.
- Set wound-covering rules: Anyone with a draining lesion should keep it fully covered and avoid shared equipment until it can be contained.
One point often gets missed. A person who is colonized but has no symptoms still needs good hygiene, because bacteria on skin or in the nose can spread through hands, towels, and direct contact. A person with an active draining infection needs stricter precautions because there is more opportunity for MRSA to move to other people or surfaces.
Facility reminder: A disinfectant wipe only works as labeled if staff use enough wipes, cover the full surface, and keep it wet for the full contact time.
Frequently Asked Questions About MRSA
What's the difference between CA-MRSA and HA-MRSA
CA-MRSA means community-acquired MRSA. It usually shows up in everyday settings such as homes, schools, locker rooms, and gyms, often as a skin infection. HA-MRSA means healthcare-associated MRSA. It is linked to hospitals, nursing homes, dialysis centers, and other medical settings where people may have wounds, devices, or frequent contact with clinical care.
The label describes where the exposure likely happened. It does not tell you how serious the infection is by itself.
Can a MRSA infection go away on its own
A small skin problem can sometimes settle down. A possible MRSA infection should not be watched casually if it is becoming more red, painful, warm, swollen, or starts draining pus.
That is where people get tripped up. Carrying MRSA on the skin or in the nose without symptoms is called colonization. An active infection means the bacteria are causing damage. If a bump is changing quickly or the person also has fever or spreading redness, it needs medical attention.
How do doctors confirm MRSA
Doctors usually start with the exam and the history. They look at how the area appeared, how fast it changed, whether there is drainage, and whether the person has risk factors such as close-contact sports, a recent hospital stay, or a recurring abscess.
To confirm MRSA, clinicians generally need a sample from the infected area for culture and antibiotic susceptibility testing. Looking at the skin can raise suspicion, but it cannot identify the germ with certainty or show which antibiotics are likely to work.
Who should be most concerned
The people who need the clearest plan are often the ones supervising shared spaces. That includes parents of athletes, school staff, gym owners, coaches, cleaning staff, healthcare workers, and anyone responsible for equipment that touches bare skin.
Concern should lead to practical action, not panic. Someone who is colonized may feel completely well but can still spread bacteria through hands, towels, razors, or uncovered skin. Someone with an active draining infection creates a higher risk because more bacteria are reaching surfaces and other people. That distinction matters. It helps you decide when routine hygiene is enough and when exclusion from play, wound covering, cleaning, and medical care need to happen right away.
Leave a Reply